



Dear Grant Illingworth KC and fellow Commissioners
I understand from your latest panui that you are currently assessing the
evidence you have gathered in order to prepare your final report. Although
the Hatchard Report submitted evidence to the Commission, our request for
a meeting with yourselves was not granted. As I was in a unique position to
offer invaluable information to the Commission, I believe an opportunity was
missed. I would like to set the record straight in a last minute sincere attempt
to serve the needs of justice.
In March 2021 immediately prior to the Covid vaccine rollout, I was
personally invited to correspond with senior individuals who had been
appointed to advise the government. These included a leading
epidemiologist, a well known business leader and a member of the Skegg
Committee. My academic background includes the use of sophisticated time
series analysis to test for causal factors in social and economic data. My
early input was well received. For example Professor Michael Baker replied
to one of my comments:
“Thank you for that very lucid description of our current state of knowledge
around Covid-19 and the uncertainties – which are large. I agree about the
importance of trying to keep an open, evidence-informed debate about future
options.”
I was well aware that mRNA vaccine technology was both novel and already
well recognised in the scientific literature to involve unique risks. Early on I
took advantage of my contacts in the global biotechnology research sector
to gather advice about these risks and to find out more about Covid origins.
There was a consensus among my contacts, who were actively doing
research on genetic medicine, that Covid originated in a laboratory, but there
was a reluctance to go public with this information for fear of losing their
position. It was also apparent that despite the known risks of mRNA
vaccination technology there was a reluctance to dismiss its use, rather my
contacts believed the severity of the early variants circulating overseas
dictated Covid vaccination should be a matter of informed personal choice.
In other words, the risks should be a matter of public knowledge and
discussion, and the effects of vaccination should be deeply researched and
assessed. This was the extent of my understanding as my correspondence
with government advisors commenced—I believed we should err on the side
of caution. Government policy was keeping Covid out of the country which
could have bought us time to assess the safety of the vaccine as it was used
overseas before we rolled it out here in NZ. In the pressured atmosphere of
the early pandemic this opportunity was missed.
It immediately became apparent to me that because NZ was almost
completely free of Covid infection, due primarily to border controls, contact
tracing and social isolation measures, we were in a unique position to assess
any effects of the novel mRNA vaccine in the absence of confounding
factors related to Covid infection. No other country in the world had this
opportunity to the degree NZ enjoyed. Therefore I took the responsibility of
my contact with senior government advisors very seriously indeed. As the
vaccine rollout began, I monitored published scientific papers on Covid and
used my data skills to assess any vaccine effects.
Early on I pointed out that lifestyle factors including diet and exercise, and
alternative medical strategies to combat comorbidities could critically affect
Covid outcomes and should be a factor in government policy to ensure a
satisfactory long term public health outcome.
But over the second quarter of 2021, as the vaccine rollout gathered pace,
my correspondence with government advisors revealed that there was an
overwhelming consensus that vaccination would contain Covid, despite the
fact that overseas Covid data was not supporting this contention. By July a
number of studies and assessments in USA and Israel (with 59% of the
population vaccinated at the time) revealed that Covid vaccination did not
stop transmission and that any effectiveness at preventing hospitalisation fell
dramatically within 10 weeks of vaccination and disappeared entirely within
180 days.
The reaction of the government team was instructive. A member of the
Skegg Committee wrote to me suggesting that Covid was being spread in
the general population by children who at that stage were not yet
vaccinated. This suggestion did not have any supporting data, it merely
reflected a predetermined policy to get everyone vaccinated as soon as
possible. I wrote back warning about the dangers of an overconfidence in
Covid vaccination that did not fit the actual data.
In August a preprint paper reported that the natural immunity acquired
through Covid infection was 13 times more effective at preventing reinfection
than Covid vaccination in the absence of prior infection. I circulated this
among government advisors. The Skegg Committee member wrote back:
“A protective immune signature is often elusive and vaccines are actually
quite primitive in design, and often don’t need to be anything other than that.
For covid vaccination, we are actually still in the first generation and there will
be lots of improvements – to dosing, dose interval, boosting and adjusting for
variants. The fact that one has to give them to everyone to protect the few
from falling victim (death) is unlikely to ever change I wouldn’t have thought.
And the chances of other ‘interventions’ having anything like their protective
effect is remote in my view.”
In other words, even though data was showing that mRNA Covid shots were
not proving effective, there was such a deep seated faith in the principle of
vaccination that the actual data and the novel nature of mRNA vaccines was
being ignored in the expectation that vaccine developers would get it right in
the end. But by September it became clear that data showed Covid
vaccination was not preventing deaths. I emailed the government team:
“I ran a linear regression for 190 countries between percentage of the
population vaccinated and deaths per million during the last seven days. There is no significant correlation (+0.034)…..I believe this points to a general
principle that: it is factors and policies other than vaccination which
primarily affect outcomes in a nation. Determining those factors is critical
in understanding the pandemic and its possible solutions. From this point of
view I am increasingly of the opinion that the current government messaging
is becoming misleading. The majority emphasis on vaccination targets is
giving the impression that a high level of vaccination alone will guarantee
freedom from Covid.”
My early correlation finding was subsequently supported by a published
study. The Skegg Committee member wrote back to me:
“I think you are right that studies have also shown that high vaccine coverage
will not alone contain outbreaks. And that, given our still low 2-dose vaccine
coverage, we are presently in a very risky situation.”
In other words, in his opinion the solution to the lack of Covid vaccine
effectiveness was more frequent mRNA vaccination. This did not appear to
make sense, especially as reports of high rates of vaccine adverse effects
were multiplying. Studies were beginning to be published showing that the
risk of Covid infection for younger age groups was very low but the risk of
adverse effects of Covid vaccination might be higher. These were red flags
which were being ignored here in NZ.
In October I received a reply from the Skegg committee member to my
concerns about a teenage girl who had died suddenly following Covid
vaccination. He dismissed this as a likely adverse effect of the oral
contraceptive, not a possible effect of Covid vaccination. I raised other
similar cases of sudden death following Covid vaccination but by the end of
October I was excluded entirely from email interaction with government
advisors. My input was cancelled. By this time the government was set on a
policy of vaccine mandates, despite the growing evidence of harm. Universal
Covid vaccine mandates for some professions and movement restrictions on
the unvaccinated were extended during November. At this point I believed
there was an overwhelming public interest to raise my voice, to go public
with my concerns and put analysis of NZ Covid data on a scientific footing.
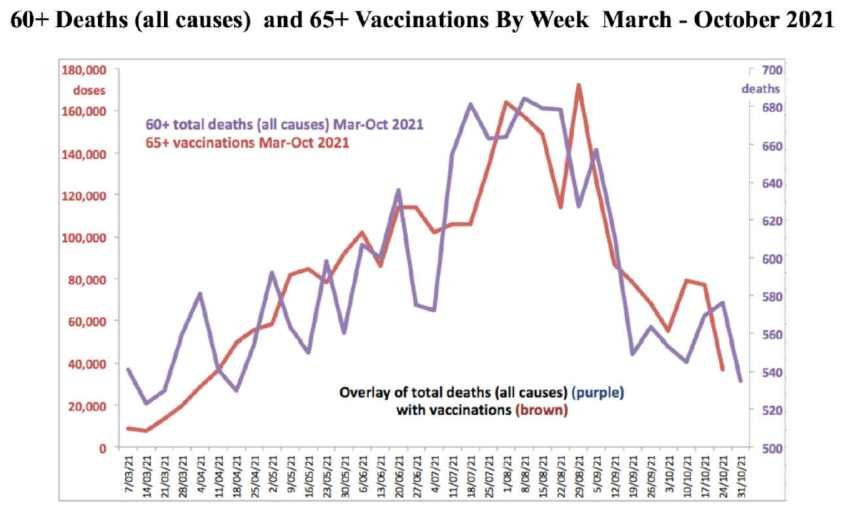
Data for weekly all-cause deaths by age was available. Weekly Covid
vaccine totals by age were being announced. It was therefore possible to
undertake a time series analysis to determine whether increases in vaccine
rates were followed by increases in deaths. I undertook this analysis for the
60+ age cohort. I compared weekly vaccination numbers in New Zealand
with weekly deaths (all causes) for the 60+ age group between 7 March 2021
and 31 October 2021. This period corresponded to the exclusive roll out of
the Pfizer Covid-19 vaccine. There were very few cases of Covid-19 active in
the community during this period and therefore the effect of the Pfizer Covid
vaccination could be studied largely free of the confounding factors of Covid
deaths. My time series analysis found a positive effect of vaccination on
deaths (all causes) at a lag of one week (t(33) = 1.74, p = 0.045 one-tailed).
Tests showed the results cannot be plausibly attributed to spurious
regression due to nonstationarity. The analysis found that vaccination was
associated with 434 additional all cause deaths during the week following
vaccination among individuals aged 60+. This age cohort received a total of
2.8 million vaccine doses during the experimental period. The finding of
additional deaths is roughly consistent with available reports of all cause
deaths proximate to vaccination that were reported. The full text of the
analysis is available at Research Gate
There are limitations to this analysis. There is no doubt that the collection of
vaccination totals by week would have been to an unknown extent subject to
haphazard data collection and recording due to the rush involved, but any
existence of a relationship between Covid vaccination and all cause mortality
in the absence of Covid infection should have been a red flag. Moreover the
possible association should have been obvious even to a casual observer of
the above graph which was widely publicised at the time and fully available
to those in government and the medical establishment who should have
been assessing the possible effects of the Covid vaccine rollout.
As many others will have pointed out to you, the government became tardy
in publicly acknowledging the risks of Covid vaccination. For example it was
not until fully six months after the risk of myocarditis and pericarditis was
well known in scientific literature that Dr. Ashley Bloomfield wrote to DHBs to
warn them. The failure to alert the public to proven risks had dire
consequences. In 2022 a prospective study in Thailand found 30% of
teenagers suffered adverse cardiac symptoms following mRNA vaccination.
In April 2023 we reported data from the Wellington region showing an 83%
increase in hospitalisation for heart attacks. In 2024 we reported a
staggering increase in ED visits for chest pain among people under 40 and a
188% rise in mortality risk among NZ teens following Covid-19 vaccination.
More recently, high quality large population studies have found relatively
higher cancer rates among the Covid vaccinated compared to the
unvaccinated. In 2025 our St John ambulance emergency calls remain at
record highs, 60% above pre-pandemic levels. Health insurance premiums
have doubled over the same time frame. Our health system is overwhelmed.
These alarming health statistics result from some key mistakes that were
made in the early years of the pandemic that could have been avoided which
I summarise as follows:
A. There was a failure to take account of the known character and depth of
the serious risks posed by novel genetic interventions as used by the Covid
vaccines. The adverse outcomes of past gene therapy trials and the results
of prior animal studies were ignored. Warnings of some internationally
prominent microbiologists were wrongly dismissed as conspiracy theories.
B. Instead, authorities followed a policy which naively and wrongly assumed
the risks and possible adverse effects of mRNA vaccines were similar to
prior traditional vaccines. In this way they limited the number and type of
conditions which might conceivably be related to Covid vaccination. They
dismissed as unrelated high rates of red flag adverse vaccine reactions
including neurological effects, kidney damage, immune deficiency,
psychological effects, cardiac issues and sudden deaths which were
occurring at unprecedented high frequencies.
C. The absence of any studies of the longer term effects of Covid vaccines
should have led to rigorous pharmacovigilance monitoring. Instead
authorities assumed that any adverse effects would only surface during the
first 21-30 days following vaccination, thus crippling their potential to assess
and understand potential Covid vaccine outcomes including cancers. Border
controls and contact tracing largely excluded Covid infection in NZ during
2021, giving NZ a unique opportunity to assess the effects of Covid
vaccination in isolation from Covid infection. This opportunity was lost.
D. Authorities actively sought to suppress and discredit those asking
questions and raising concerns on both local and international platforms,
including valid scientific results and discussions. They made repeated public
assurances of safety and efficacy in the face of contrary evidence and
sought to control media and social media content and discussions,
apparently in order to suppress Covid vaccine hesitancy. They severely
disciplined doctors offering informed consent.
E. The government sought scientific advice mostly from committed vaccine
advocates who had a very limited understanding of gene technology. They
too readily accepted the clearly biased communications from Pfizer advising
safety and positive trial outcomes. Crucially, ignoring the alarming details of
wide scale high frequency adverse events contained in the document 5.3.6
Cumulative analysis of post-authorization adverse event reports of Pfizer
bnt162b2 received through 28-feb-2021, a version of which our government
received in 2021 and whose implications have been thoroughly analysed in
the published scientific literature.
F. In assessing the massive volume of scientific publishing on Covid-19
which runs to many more than 100,000 papers, there was a failure to take
account of the known hierarchy of evidence. The results of prospective
studies, time series analysis, studies of large populations, studies comparing
outcomes of vaccinated and unvaccinated populations and studies
examining longer term outcomes should have taken precedence. If this had
been followed, dangers would have been apparent and problems averted.
G. As time went by and evidence of harm in the population both here and
overseas began to accumulate, authorities attempted to limit access to key
NZ source data especially concerning specific parameters such as vaccine
status, cardiac disease, cancer, excess mortality, etc. Those figures that
remained accessible or were leaked, painted a very grim picture of
accelerating ill health since 2020 that continues to be ignored by Health NZ
or erroneously blamed on factors that have remained largely unchanged
since 2020. Yet it has become ever clearer that the rate of Covid vaccine
injuries reported to CARM is only the very tip of the iceberg. A Covid death
whistleblower Barry Young is still facing prosecution. Doctors raising
questions about Covid vaccines are still being censored
It is apparent that long term public health outcomes have been harmed by
the combination of Covid infection and vaccination. Both of these almost
certainly resulted from biotechnology experimentation. The failure of the
government and Health NZ to come to grips with the implications of the
health data needs to be exposed and discussed publicly. Your role as
Commissioners requires a full examination of the scientific data that has
been so far ignored here in NZ. I remain available to discuss these issues,
they are within the Commission’s terms of reference. They should not be
omitted from your final report. This is a matter directly affecting public health
and longevity.
Yours sincerely
Guy Hatchard PhD
Guy Hatchard PhD Biography
Guy Hatchard is the creator and principal contributor to the Hatchard Report.
He has been a life-long advocate of food safety. He was formerly Director of
Natural Products at Genetic ID, a global food safety testing and certification
company now known as FoodChain ID. Genetic ID developed techniques to
test for the presence of genetically modified organisms in food and provided
services to bulk food trading companies like ADM, Cargill, and many others
in order to facilitate access to export markets and increase consumer trust.
He has presented his findings to governments and industry leaders around
the world. He appeared before the NZ Royal Commission on Genetic
Modification and has been a key figure in discussions since 2017 which
eventually led to the repeal of the Natural Products Bill. He has written a
book Your DNA Diet which is available from Amazon.
He received his BSc Hons. from the University of Sussex, UK, in Logic and
Theoretical Physics with a special focus on the scientific method. He
qualified with a Certificate in Teaching from Canterbury Teachers College,
Christchurch. His MA thesis at Maharishi International University (MIU), Iowa,
analysed outcomes of mastery learning in Mathematics. His PhD thesis in
Psychology at MIU investigated the impact of human factors on national
competitive advantage using time series analysis. Maharishi International
University (MIU) is fully accredited by the Higher Learning Commission (HLC)
which is recognised by the US Department of Education and the Council on
Higher Education Accreditation (CHEA). It incorporates principles of
consciousness-based education (CBE). CBE includes traditional subjects
while also cultivating the student’s potential from within. He has published
papers in peer reviewed journals and was the keynote speaker at the 1996
annual conference of the British Psychological Society on Crime.

{kind=link}