



Over the last few weeks the Hatchard Report has been discussing high rates of excess all-cause death around the world.
The connection with Covid vaccination is statistically evident and the evidence is mounting. This is not only affecting the aged but also young and working age people. Rather than rehashing the arguments you can catch up via this substack article which explains how the emerging data on injury and death is becoming too hard to ignore.
The high rate of all-cause deaths, some of which are sudden and unexpected, has increased the workload of coroners. Dr. Judy Melinek is a US coroner who moved to New Zealand in 2020 to take up a position in Wellington. An extract from her 22 August 2022 blog at Medpage Today illustrates the challenges coroners face:
“The Ministry of Health, meanwhile, has changed how they count COVID-19 deaths, distinguishing who is dying of COVID-19 and who is dying with COVID-19. I’m a professional who has to make legally-mandated decisions about these kinds of things, and even I am struggling to parse that policy. Here’s a hypothetical example drawn from several cases I’ve done recently. A young adult man comes to my autopsy table. He had been apparently healthy and died suddenly. When I open him up, there’s nothing inside — no gross anatomic findings on autopsy that would explain his death. Under the microscope, however, I do find evidence of scarring in the heart tissue. When the body came to the hospital and then into our mortuary, he had two COVID-19 PCR swabs; one came back positive and one came back negative. So, we can surmise that this dead guy is harboring a low viral load — but is that an indication of a recent, healing infection or a “historic,” remote one? And how does it play into the cause of death?….
“Too many what-ifs. In my field, we don’t like what-ifs. We’re supposed to provide final answers to coroners and to the decedents’ families. Knowing that what I write on the death certificate becomes part of the public record and actually influences the numbers our national health authorities generate makes me super cautious. I show the case to other pathologists. I schedule a peer review. I do extra stains and tests for viral PCR on the tissue — tests I would not have had to run 2 years ago — and I agonize over every word in the opinion on my autopsy report. Even routine cases for a forensic pathologist, like motor vehicle accidents and drug overdoses, get extra scrutiny if they test positive for COVID-19, or if they received a vaccination and the family or coroner wants me to answer whether the death had something to do with that.”
Dr. Melinek is certainly a Covid vaccine supporter and has given public interviews decrying conspiracy theorists and anti vaxxers, but her report indicates that key decision makers at the pathology end of all-cause deaths are sometimes unsure and becoming super cautious.
Others are making up their minds. Dr. Alex Washburne is a mathematical biologist and the founder and chief scientist at Selva Analytics. He researches Covid epidemiology, the economic impacts of pandemic policy, and stock market response to epidemiological news. He wrote on Twitter yesterday:
“As the dominoes fall, there’s a very real chance that the people we thought
heroes in the pandemic were actually villains. There’s also a real chance the researchers with the most-cited papers are actually guilty of the worst research misconduct of the century.”
There is an interesting contrast here between someone who cuts up dead bodies and looks for clues and someone who analyses public Covid data and advises financial markets. The one becoming more cautious, the other becoming more suspicious.
Pathologists are not trained to analyse social data, and epidemiologists are not trained to examine internal organs, but given the complexity and novelty of the pandemic they certainly need to listen to each other very carefully.
Primary Data Sources are Very Important
Both of them are dealing with primary data sources, which brings us to a huge problem with the formation of the pandemic response policy. A lot of policy is being formulated based on out-of-date secondary and tertiary sources which no longer match up with primary data sources.
The primary sources are objective data sets from both research projects and public data collection. Some of these may involve subjective judgements on the part of physicians, but let’s hope that these are made carefully as Dr. Melinek reports she does.
Secondary sources involve published analysis of the data sets. These are scrutinised through peer review both formally and informally, but as Dr. Washburne reports even these can be subject to bias and misconduct. However, inconsistencies and inaccuracies, whether unintended or not, usually surface as time goes by, as evidenced by the 500+ drugs released then withdrawn from the market since 1950.
Tertiary sources involve administrative decisions taken by health advisors and experts. These are further from the primary source data and can involve professional bias. We have certainly seen a lot of this during the pandemic.
One step further away from the data, politicians and media explainers make their own assessments, advocate policies, and relay these to the public. We are now many steps away from up-to-date information in the rapidly evolving Covid data landscape. Political and commercial agendas are being funded in the media. Huge mistakes can and are being made. Mistakes that are evidently costing lives, as the rising excess all-cause death data shows.
This recent answer from the Green Party in the Rural Greens blog in response to the coronial inquest into a death attributed to mRNA vaccine side effects illustrates this point:
“Thousands of lives saved, one death in over 4 million vaccinations not even counting the boosters. You could hardly avoid all the information on the ministry website, articles in Stuff, TV and radio. This is sad for the family, just as it is sad for those families who lost completely healthy people to Covid world wide. Let us be clear once and for all, the Green Party is encouraging all sorts of vaccinations because they have proven to be effective and in some cases leading to elimination of diseases.”
In other words, this Green Party spokesperson relies on tertiary sources and MSM. They even got the Ministry of Health’s advice wrong, assuring us that there has been only one death in New Zealand as a result of mRNA vaccination—a preposterous assertion incompatible with primary data.
Political posturing like this has hardened public opinion, but it has done little to foster real understanding of the risks.
Effects of mRNA Interventions can be Inherited
The pathologist and the epidemiologist (as well as the Green Party spokesperson) we have already met, might do well to talk to the geneticists who published on 20th August 2022 a paper entitled “Pre-exposure to mRNA-LNP inhibits adaptive immune responses and alters innate immune fitness in an inheritable fashion“.
This is a study of the effect of Lipid Nanoparticles (included in Covid mRNA vaccines to facilitate the entry of genetic information into cells) on immune system function in mice. It concluded
“In summary, the mRNA-LNP vaccine platform induces long-term unexpected immunological changes affecting both adaptive immune responses and heterologous protection against infections. Thus, our studies highlight the need for more research to determine this platform’s true impact on human health.”
In other words, whatever mRNA vaccine achieves, good or bad, it could be passed on through generations. A frightening prospect—mistakes may never go away and could haunt future generations.
How can Pathologists Accurately Determine the Cause of Pandemic Deaths?
After the autopsy, what is a cautious pathologist going to write down when it comes to describing the cause of an unexpected death in the time of Covid?
Firstly, there is no requirement to record vaccination status on the death certificate, so a vital primary source of data is being discarded. Secondly and crucially the actual ‘cause of death descriptions’ that a pathologist has to choose from are limited by training and prior experience. There hasn’t been a mass use of genetic vaccines before the pandemic—so they are not recognised as a cause of death in the normal course of things.
Let’s illustrate the dilemma pathologists face. This is part of a diagram I used when lecturing at university. It is designed to simply illustrate the key role of DNA in orchestrating all parts of the physiology:
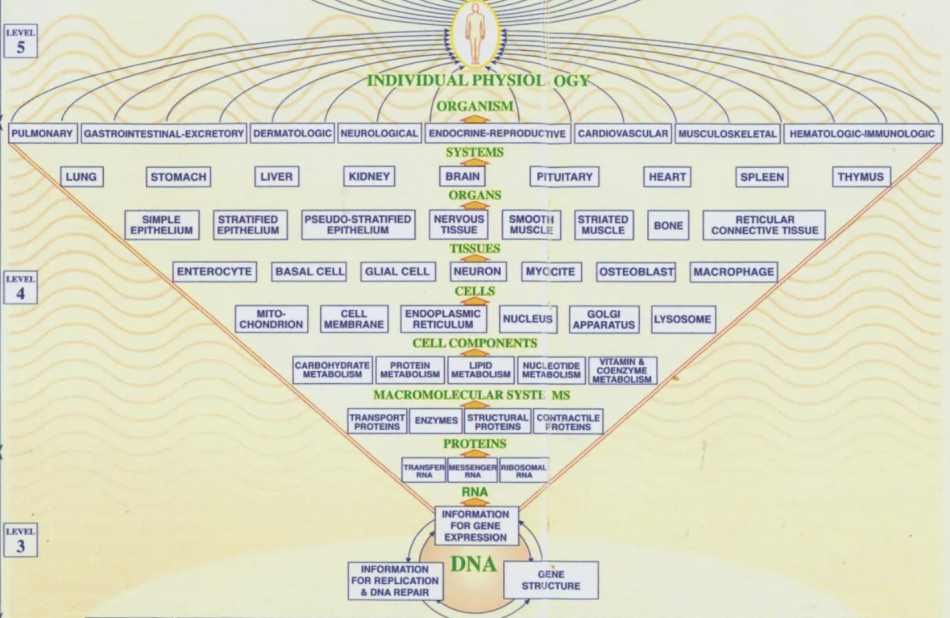
The complexity involved in physiology is immense, but the hierarchical dependence on the information contained in DNA and its expression through RNA is obvious. Modify the RNA pathways through which DNA expresses itself, and you can see that every level of physiological function can potentially be affected.
As you go up this chart from levels 3 to 4 to 5, you reach larger time and distance scales which can be observed by a pathologist with the naked eye or through a microscope. Go down the chart, entities are smaller and cycle more quickly, they are not visible to the naked eye (levels not shown here below DNA are the areas covered by physics).
The pathologist is mainly examining organs and tissues (the higher elements of level 4). Post mortem test options are limited, although pathologists do have access to medical history and the results of tests conducted during life. There is no question of being able to examine the specific role that genetic manipulation (Level 3) might have played in any death. Pathologists don’t have the genetic expertise or the tools to determine this.
Nor is there any precedent to indicate this might be at issue. Mass human mRNA vaccination is novel, so pathologists are in almost completely uncharted territory. Not only that, but they have been constantly bombarded with assurances that mRNA Covid vaccination must be safe, by definition. Assurances that primary data is now calling into question.
In a prescriptive medical professional environment, no pathologist is going to risk writing an autopsy report that implicates Covid vaccination (unless it involves an absolutely clear cut unambiguous case of myocarditis without any history of Covid infection). To express doubts or to pass judgement on the role of genetic interventions is outside of their expertise. To do so could result in professional censure and possibly loss of employment.
Yet the primary data shows mRNA vaccination is associated with high all-cause death rates beyond historical levels. The unvaccinated are not suffering in this way. The inevitable question—is there a causal connection between mRNA vaccination and a very large number of deaths?
mRNA vaccination inserts a set of genetic instructions into cells that overrides the highly regulated cellular environment and stipulate the production of Covid spike proteins. We can term this ‘genetic dysregulation’.
It appears that the consequent stimulation of the immune system to respond to the Covid spike protein can lead to immunosuppression that increases with each subsequent vaccine dose. This is just one of multiple effects on physiology that are suspected, but as yet not investigated thoroughly.
Is the ultimate primary cause of death of a great many persons: ‘genetic dysregulation brought on by mRNA vaccination’? If so, there is no such standard box for a pathologist to tick and no one currently involved in certifying cause of death who could possibly attest to this.
Genetic dysregulation, or we could use the term ‘immune deficiency contingent on mRNA vaccination’, can underlie multiple symptoms and multiple disease types. High cancer rates, heart disease, bacterial infections, stroke, kidney disease, and neurological conditions can all be related to a single cause—the action of genetic vaccines at the all-powerful time and distance scales of genetic functioning.
It is not unscientific to suggest that multiple conditions can have a single cause. Hans Selye, an eminent Canadian scientist, popularised the notion that ‘stress’ contributes to a range of illnesses. He termed stress “the non-specific response of the body to any demand placed upon it”.
In the same way, sooner or later, primary data linking high all-cause death rates with mRNA vaccination must lead to a serious examination of ‘genetic dysregulation’ as an underlying cause of death. This is not a new suggestion. Italian researchers proposed post-mortem procedures to identify causal adverse effects of Covid vaccination in May 2021. However, this has had little or no effect since on autopsy procedures. This is because of the entrenched preconception that all vaccines, including novel biotech vaccines, will be safe. A preconception still shared by most medical professionals.
The geneticists, the epidemiologists, the pathologists, the administrators, and the politicians are not talking openly and honestly to one another or to the public. If they are aware that primary data shows all-cause deaths are related to mRNA vaccination, they are not talking about it, but are busy looking the other way and hoping no one will blame them. Some appear to be making sure that vital primary data is kept well hidden.
Growing evidence of serious long term Covid mRNA vaccine health risks, should be telling us that lives are at stake, many lives. The implications for public policy should be obvious, medical interventions designed to alter genetic expression and function are highly unpredictable and very risky. They can have powerful effects widely distributed in physiology.
Therefore novel biotechnology experimentation designed to create new pathogens or alter genetic function needs to be paused, and quickly. Any form of Covid vaccination mandate, public or private needs to be outlawed immediately. Covid vaccination programmes should be halted, as has happened in Denmark for the young.
Guy Hatchard Ph.D. was formerly a senior manager at Genetic ID a global food safety testing and certification company (now known as FoodChain ID)
Guy is the author of Discovering and Defending Your DNA Diet

{kind=link}