A May 31st report in the Guardian entitled “Three jabs best for preventing Covid infections, global analysis finds” reports on a study published by the BMJ on the same day.
The authors searched global World Health Organisation (WHO) databases in an effort to discover whether mixing and matching vaccine types was better than sticking to one brand.
The study concludes that a combination of any three mRNA vaccines is 95% effective against hospital admissions. It also says that even two doses of mRNA vaccine are 99% effective at preventing severe Covid.
Did the authors realise that these astonishing and entirely unconvincing headline effectiveness figures will grossly mislead and deceive the public?
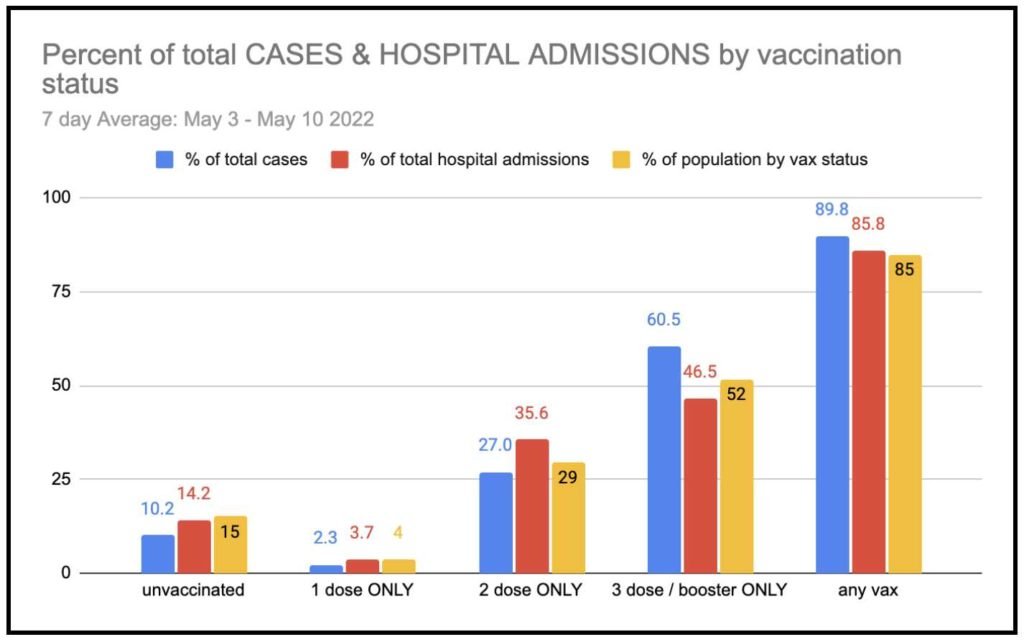
I don’t know, but I do know that real world figures from around the world show the exact opposite. At the very least, there is currently no statistical difference between rates of hospital admissions for the vaccinated and unvaccinated.
Here in New Zealand and in many other countries who still publish data, official figures show that the triple vaccinated are in fact more likely to be hospitalized with Covid. In other words, mRNA vaccination damages health.
Rigorous Scientific Enquiry is Taking a Back Seat
The paper illustrates just how far our understanding of Covid outcomes has drifted away from rigorous scientific enquiry into a self-congratulatory faith.
The Guardian report on the study begins with the phrase “the effectiveness of individual coronavirus vaccines is well known”. This must be a typo, surely the author meant to write ‘ineffectiveness’?
Hidden in the conclusion of the BMJ paper is a vital clue:
“The vaccine effectiveness against death in people who received three doses of mRNA vaccine remains uncertain”
Now correct me if I am wrong, but surely if a vaccine is claimed to be 95% effective against hospitalisation and 99% effective against severe Covid, it must prevent deaths?
Well according to the paper’s authors their comprehensive review of all WHO databases cannot confirm this. How come?
The answer lies in the interpretation of data and the use of statistics.
Whilst careful editing and curation of hospitalisation and infection data is possible, death has a finality which is hard to ignore. Mortality statistics are carefully recorded everywhere. These show that all cause mortality is on the rise.
The possible culprits are either Covid itself or Covid vaccination. Whichever is the case, the argument for the effectiveness(??) of Covid vaccination against death is a non-starter.
Vaccine proponents are out in force these days arguing (without credible evidence) that increased deaths, especially the significant increases in cardiac illness and deaths among working age people, have nothing to do with mRNA vaccines and everything to do with long Covid.
View a heart specialist in New Zealand recently commenting to this effect.
A report “Increased emergency cardiovascular events among under-40 population in Israel during vaccine rollout and third COVID-19 wave” published in Nature found to the contrary:
Emergency Cardiac Callouts Were Related to Vaccination, But Not to Prior Covid Infection
The authors concluded “It is essential to raise awareness among patients and clinicians with respect to related symptoms (e.g., chest discomfort and shortness of breath) following vaccination or COVID-19 infection to ensure that potential harm is minimized.” and further said:
It is “critical to better understand the risk-benefits of the vaccine and to inform related public policy and prevent potentially avoidable patient harm.”
Governments and Health Authorities Have Ignored the Conclusions of Evolving Covid Science Publishing
In fact, over the last 18 months, the whole mythic edifice of mRNA vaccination safety and effectiveness has come tumbling down due to new scientific findings and assessments.
So what do you do if you are a Covid mRNA vaccine proponent? Of course, you double down on your faith, you plough on regardless:
At first mRNA vaccination was 95% effective against infection and completely safe. Then it was discovered it rapidly waned in effectiveness. So it was pronounced effective against severe infection and hospitalisation.
Then it was realised a very wide range of adverse effects followed vaccination, so these were designated as unrelated or caused by vaccine anxiety.
Then the volume of myocarditis cases was too high to ignore, so these were described as mild and short lived.
Then post-vaccine myocarditis was discovered to be long lasting and potentially serious or even fatal, so it was suggested that early intervention would work well.
Then it was discovered that all cause mortality was rising, so it was suggested this must be due to post-Covid infection complications and not to vaccination.
New Zealand epidemiologist Michael Baker, a favourite of the government, is currently gaining widespread media coverage with suggestions that mRNA vaccination prevents 90% of hospitalisations and has saved 80,000 New Zealand deaths.
No doubt reassuring to the 90% of the New Zealand population who are vaccinated, but it doesn’t fly scientifically in any shape or form.
The approach of the New Zealand Government government remains unchanged by the evolution of Covid scientific publishing, note:
- Their lack of ability to change policy in the face of evolving scientific publication.
- Their lack of empathy for those suffering adverse effects.
- Their scapegoating of the unvaccinated without basis in fact.
- Their rejection of alternative approaches to health.
- Their adherence to mask wearing even though studies show it is ineffective at stopping the spread of infection and also damaging to health.
Governments and Mainstream Media are Championing Disinformation
More worrying are efforts around the world to establish so called disinformation offices devoted to
- attacking anyone who questions the safety of mRNA Covid vaccination
- issuing reassuring but patently false bulletins about Covid vaccination safety and effectiveness
The New Zealand government has joined in with “The National Centre of Research Excellence for Preventing and Countering Violent Extremism” (yes, this does appear to be concerned with the investigation of anyone doubting the safety of mRNA Covid vaccination).
For a prime example of the doublespeak of disinformation officers, try the BBC’s very own Rachel Schraer who weighed in today with a graphic presentation entitled “Covid: Why do some vaccines protect you longer than others?”.
The bright and breezy Schraer (I couldn’t find her bio online) was “very sure that the jabs are safe and effective”, but unsure exactly how long they last for—somewhere between measles and influenza jabs she hazarded.
No mention of any side effects and no mention of mRNA technology, just the reassuring generic term ‘vaccine’ and oblique references to what unnamed experts think (or possibly imagine?).
The saddest part of this is the fact that examination of the Pfizer documents gradually being released under court order shows that the adverse effects and the waning effectiveness, and much more worrying prospects such as suppression of the immune system or pregnancy complications, were known or suspected after the earliest Pfizer trial results, but hidden from the public.
It is a year since my best mate died from cardiac and immune suppression, conditions which he suddenly and unexpectedly acquired following Covid vaccination. We have not forgotten him.
Exposing the risk of genetic experimentation is still our priority. Nor have we forgotten the Wuhan Virology Lab and similar programmes around the world. Unfortunately, they have not forgotten either, recent publications show that the Wuhan lab is continuing to experiment with dangerous viruses.
Man-made viral experimental genetic material is mobile and invasive, it can reach you wherever you live. It can take control of life, your life, and change it irrevocably. Its ultimate effects are unknown and unknowable.
History shows us it cannot be safely contained in a lab indefinitely. The peril is ours, and we can’t pretend it doesn’t exist or even successfully hide from it.
We are already a long way down the road to ruin, but possibly it is still not too late to turn back. The only road back to safety involves pausing risky biotechnology experimentation immediately.