What Went Wrong and How Can it be Corrected?
Now that many governments including New Zealand have at last laid out some criteria to end mandates and vaccine passes, we ask is this sufficient to resolve the problems created by pandemic policy and prevent a recurrence?
This article starts by laying out the gist of prevalent pro-vaccination arguments in order to be able to set up a rational summary of our current knowledge concerning Covid-19 mRNA vaccination safety and set up an exit strategy by recommending measures that will help resolve the divisions in society.
Attitudes to Vaccine Hesitancy and Effectiveness
No consideration of vaccination can omit mention of the MMR and autism scandal of the nineties.
In 1998, the Lancet published a paper by physician Andrew Wakefield that claimed there was a link between the measles, mumps and rubella vaccination and incidence of colitis and autism spectrum disorders.
This paper led to much public vaccine hesitancy, but was later judged to contain misleading data and was withdrawn by the Lancet in 2010.
Whatever the merits of the case, ever since vaccination hesitancy has been linked with notions of fraud and criminal behaviour.
The discussion of this case now plays an important role in medical education, but unfortunately tends to promote an incautious attitude to vaccine safety procedures.
The MMR medical hoax has reinforced the notion that vaccination is always a social good and that vaccine hesitancy is a form of anti-intellectual, Luddite behaviour to which ill-informed people are particularly vulnerable.
A very long history of vaccination and its success in reducing the impact and elimination of some diseases such as smallpox have led to trust and reliance that places vaccination at the forefront of preventive medical strategies with a presumption of safety.
Medical literature has grown up which discusses the psychology of vaccine hesitancy and dismisses adverse effects of vaccination as predominantly a nocebo effect due to anxiety and mass hysteria.
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC8483981/
It is this perspective that has dominated the discussion of Covid-19 adverse effects in the world.
It is particularly noteworthy that the David Skegg committee here in New Zealand was almost exclusively composed of experts in epidemiology, a profession who would largely share this perspective as one of their core values.
There is an understanding in the epidemiological field that vaccination is the preferred solution to communicable disease which will ultimately be sufficient to control its spread.
For example, Philip Hill, McAuley Professor of International Health, Co-Director, Centre for International Health, Department of Preventive and Social Medicine, Otago Medical School, wrote to me on 1st September 2021
“A protective immune signature is often elusive and vaccines are actually quite primitive in design, and often don’t need to be anything other than that. For Covid, we are actually still in the first generation and there will be lots of improvements – to dosing, dose interval, boosting and adjusting for variants. The fact that one has to give them to everyone to protect the few from falling victim (death) is unlikely to ever change I wouldn’t have thought.”
Professor Hill could not have been aware of just how much of a structural break in vaccine methods the novel mRNA technology represented.
Like most medical professionals busy and isolated in their work environment, he would have been limited by exposure to rosy commercial biotechnology PR which was promising more exact techniques and outcomes in its search for funding.
As a result, he would not have anticipated the public health disaster of Covid vaccine adverse effects that was beginning to unfold.
He shared the medical profession’s acceptance of vaccine safety.
In fact, the very misuse of the term ‘vaccine’ to describe a novel experimental intervention was a source of reassurance.
The inside story among gene therapy researchers was far different from this.
Underwhelming and mutagenic outcomes were still plaguing animal and the few human trials approved.
For a discussion of the key issues, with references, see my video The Pandemic of Biotechnology:
Among the general public, pro-vaccination attitudes can be somewhat extreme and vary greatly in intensity.
At one end of the spectrum of opinion, especially since the start of the Covid pandemic, the notion has been passed around that unvaccinated individuals and those that refuse to have their children vaccinated are nothing more or less than murderers.
At the other end there are fears that unvaccinated individuals are unnecessarily using up healthcare resources by failing to protect themselves and others from sickness.
Pro-vaccination ideas have especially curated mainstream media attitudes to publishing.
For example, I received this message from Jesse Mulligan popular host of Afternoons on RNZ on 6th December 2021
“I enjoy some of your observations but I’m worried that you appear to line them up in a way that makes people lose perspective around the vaccine. I feel like anybody aiming to critique such an obviously positive public health measure should begin and end their messaging reminding people that any risks/flaws in the vaccine are minor compared to the horrific impacts of getting covid. I think your messages would be better received by the scientific/media community if that were the case.I don’t have the time to correspond with you on this at length but, for what it’s worth. If you’re putting people off getting a largely safe vaccine by what you’re writing about it, I think you need to review how you approach writing these messages.”
Note the “obviously positive” epithet ascribed to vaccination that is contrasted with the “horrific impacts” of Covid.
If you solely used mainstream media and government messaging as your sources of information, the foregoing discussion of Covid and mRNA vaccination would sit easily with you and ring true.
Jesse concludes by ruling out any public messaging that would put people off Covid vaccination.
This certainly chimes exactly with government messaging.
Does this conclusion stand up to scrutiny as Jesse suggests it obviously does?
Science and New Zealand Vaccine Policy—Impacts
The arguments for the safety and efficacy of vaccination, in general, underpin policies that enforce Covid-19 vaccination through restrictive mandates, but this simple narrative falls apart to a large extent when you look at Covid-19 science journal publishing.
This is a huge field.
I have a list for example of 1000 papers that deal with adverse effects of Covid-19 vaccination, and this is only a small part of the published literature.
New journal papers are coming out at an unprecedented rate.
The David Skegg Committee recommended that the New Zealand government undertake regular formal reviews of new pandemic scientific publishing to ensure its policies remain up to date.
I see no evidence that this has happened to any extent compatible with good faith.
Thus those busy people who rely on sources like Twitter and mainstream media digests for their information can be completely misled about the import and significance of Covid science publishing.
I summarise here only a few considerations which point to a divergence of government policy from published data and established medical safety protocols and ask ‘What are the human impacts of the unwavering application of New Zealand Covid vaccination policy as it was first formulated?’.
1. Children, teens and young adults are at low risk of harm from Covid-19 infection but at a relatively high risk of harm from mRNA vaccination.
The published arguments are complex, with many papers coming down on either side.
Crucially there is no mainstream consensus, advice is equivocal. See this recent paper in BMJ:
https://adc.bmj.com/content/107/3/e23 (link updated July 2022)
Conclusion: In the absence of published definitive data, incentives that coerce children to vaccinate by reducing opportunities to participate in social activities are in clear violation of the human rights of children to avoid quantifiable medical risk if they or their parents decide to do so.
2. It is no longer rationally and empirically arguable that vaccination significantly reduces transmission and infection (despite continuing reports in mainstream media to the contrary).
There is a huge volume of published data on this topic.
See this recent summary for example in Nature: https://www.nature.com/articles/d44151-022-00010-y
The situation is complicated by the fact that any marginal protection from mRNA vaccination wanes very rapidly, but also exposes vaccine recipients to additional risk.
Please note that most recent data from many countries including the United Kingdom and New Zealand point to at the very least proportionately equal rates per 100,000 of infections among both the vaccinated and unvaccinated.
This undermines prior justifications for mandates.
For a full discussion of the most reliable of recent paper on Omicron data see:
This paper which follows 50,000 subjects indicates that Omicron hospitalisation and death rates are very very low (lower than influenza).
Moreover, outcomes are similar for both vaccinated and unvaccinated.
3. The genetic techniques used in mRNA vaccines pose additional risks
It was established in the last quarter of 2020 that genetic sequences contained in both the Covid-19 virus and the mRNA vaccines can and do integrate into the human genome.
https://www.biorxiv.org/content/10.1101/2020.12.12.422516v1
This is a crucial argument.
It places Covid-19 vaccination in a special high risk category that individuals have a right to avoid if they so wish.
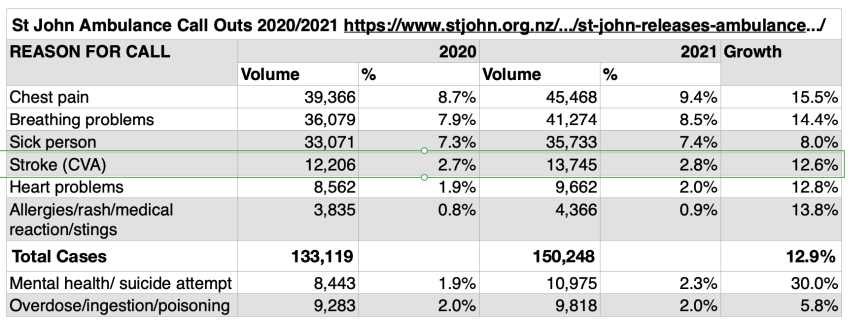
The fact that adverse effects reported to Medsafe are running at 30 times the rate of flu vaccines is supportive of a sea change in the level of risk introduced by mRNA biotechnology techniques.
4. Mandatory reporting of Covid-19 vaccine adverse effects should have been instituted.
Even though mRNA vaccines went through only a short testing period of less than one year from which key phases of 10 year testing normal to vaccination safety protocols were omitted, the Ministry of Health has refused to institute mandatory reporting of adverse effects of the Covid-19 vaccination and continues to do so.
I have received two written communications to this effect from Dr. Astrid Koornneef Director, National Immunisation programme, writing on behalf of Dr. Ashley Bloomfield (one in December 2021 and one on 15 February 2022).
Koornneef admits:
“In some countries it is mandatory for healthcare professionals to report adverse reactions in specific circumstances, however New Zealand has a good reporting culture for adverse reactions in general.”
In other words: business as usual, no special procedures are necessary for a novel biotechnology approach that hasn’t been properly tested.
Our faith in vaccination is undimmed.
Critically, phases of testing designed to catch secondary medical effects of mRNA vaccination have never taken place.
Without mandatory reporting, there is no way any valid statistical constructs of safety can be constructed, the more so because Medsafe itself estimates just 5% of adverse effects are reported in New Zealand.
Nor can valid comparisons of adverse effect rates with population norms be made.
In addition, the total absence of long term testing of Covid-19 vaccines points to an obvious need for caution when applying vaccine mandates that have been ignored.
5. Adverse effects of Covid-19 vaccination are at least 30 times higher than those of traditional vaccines.
The situation of those many individuals seriously affected by mRNA vaccination is dire.
Government messaging on the topic is deliberately reassuring but short on detail.
The latest Medsafe report on adverse effects was issued on 16 February 2022:
https://www.medsafe.govt.nz/COVID-19/safety-report-40.asp
This reports a tsunami of almost 52,000 adverse effect reports (remember that according to Medsafe these are grossly under reported).
Of these 147 were deaths.
Following medical assessments by CARM and Medsafe it was determined that:
- 60 of these deaths are unlikely related to the COVID-19 vaccine
- 64 deaths could not be assessed due to insufficient information
- 21 cases are still under investigation.
- 2 deaths were likely due to vaccine induced myocarditis (awaiting Coroner’s determination)
These Medsafe determinations appear extraordinarily vague.
Prior to the pandemic medical protocols and ethics would have required the vaccination programme to be suspended pending full investigation of deaths.
Medsafe’s summary report comparing adverse effect data with population norms is statistically invalid due to inadequate reporting.
See my article “How Medical Ethics Came To Be Ignored”
There are 2460 reports of adverse effects judged by Medsafe to be serious.
Were the affected individuals able to escape further Covid-19 vaccination through exemptions?
The New Zealand Ministry of Health criteria for medical exemptions are at:
https://www.health.govt.nz/system/files/documents/pages/vaccine-temporary-medical-exemption-30nov21.pdf
UPDATE: It looks like the Ministry of Health has removed the medical exemptions page – Sorry – you don’t have permission to access this page on our server.
These are incredibly restrictive, a maximum duration of six months is allowed and all those being granted a temporary exemption are expected to eventually complete their vaccination in consultation with their medical practitioner.
Dr. Ashley Bloomfield alone has the power to grant exemptions.
Information about the number of exemptions granted and refused is hard to access, but exemptions are certainly few in number.
6. Social Media Reports
Due to Medsafe’s restricted and veiled discussion of adverse effects, there is only one way to access individual experiences—through social media.
Since many normal channels to ask questions are blocked by either mainstream media, medical or political indifference, social media has become a place of last resort for New Zealanders.
For example on 17 February 2022 the Health Forum NZ which has 35,000 members posted a question on its FB page: “MEDICAL EXEMPTION Have you been granted a medical exemption for the Covid vaccine from Ashley Bloomfield? If so, on what grounds were you successful?”
There were 476 comments indicating extreme reluctance and mostly refusal on the part of the New Zealand Ministry of Health to grant vaccine exemptions to those already injured by their first jab.
Conclusion
Government policy has been largely formulated in the context of scientific publishing that is in many cases now outdated.
Moreover, political bias in science publishing appears to have affected its formation.
For example, see my article ‘The Jacinda Papers’
How did the government fail to properly investigate the mounting evidence of vaccine harm?
Why did the Prime Minister delete more than 30,000 reports of vaccine harm from her FaceBook page without instigating an investigation?
How did the government come to push pre-pandemic notions of vaccine safety into the discussion of biotech vaccines without a comprehensive safety assessment?
Did the Prime Minister feel along with pro-vaccination advocates that this was a now or never moment when vaccination compliance would be pushed to its limits whatever the circumstances and casualties?
There is a need now to review policy in order to take account of a broader consensus of recent Covid-19 science publishing.
There is also a need to review the impacts of government vaccine policy on both individual health circumstances and age cohorts.
In the light of the high rate of adverse effects of Covid-19 vaccination, safety protocols need to be updated and strengthened.
There is time needed to scientifically assess how much of pandemic injury is due to Covid and how much is due to vaccination.
To allow time to review and effect the needed reforms, there needs to be an immediate pause on mandates.
Nations have been so polarised by pandemic policy and misinformation, there is also a need for a period of mature and collective national reflection along the lines of a truth and reconciliation commission.
The process of acknowledging fault and designing procedures to safeguard against future mistakes is the sine qua non of resolution.
Guy Hatchard PhD was formerly a senior manager at Genetic ID a global food testing and certification company (now known as FoodChain ID)
Guy Hatchard has written a book Discovering and Defending Your DNA Diet.