




This is the first of a series of reflective articles for publication on Covid data and causality.
I note that the Ministry of Health Covid-19 Science Updates web page is now eight months out of date.
The advice it offers is in many respects outdated and superseded by events and more accurate scientific assessments.
I know that you will realise the importance of keeping up with analysis.
Media Representatives, the following report is available as a PDF document, click here to view and or download A Report on the Interpretation of Covid-19 Pfizer Vaccine Safety
Data Report:
Is the Analysis of the Pfizer Covid-19 Vaccine Outcomes Data a Case of Misdiagnosis and Medical Misadventure?
The Medsafe report Adverse events following immunisation with COVID-19 vaccines: Safety Report #39 – 31 December 2021 lists 46,000 adverse events reported since the start of the Pfizer vaccine rollout in New Zealand.
Historically this is 30 times the rate of adverse effects reported for flu vaccines. More than 50% of these adverse effects are reported by medical professionals and about 40% by affected members of the public via the CARM (Centre for Adverse Reactions Monitoring) website.
Prior experience published by Medsafe concludes that only 5% of adverse events are reported to CARM. A total of 8.1 million doses have been administered.
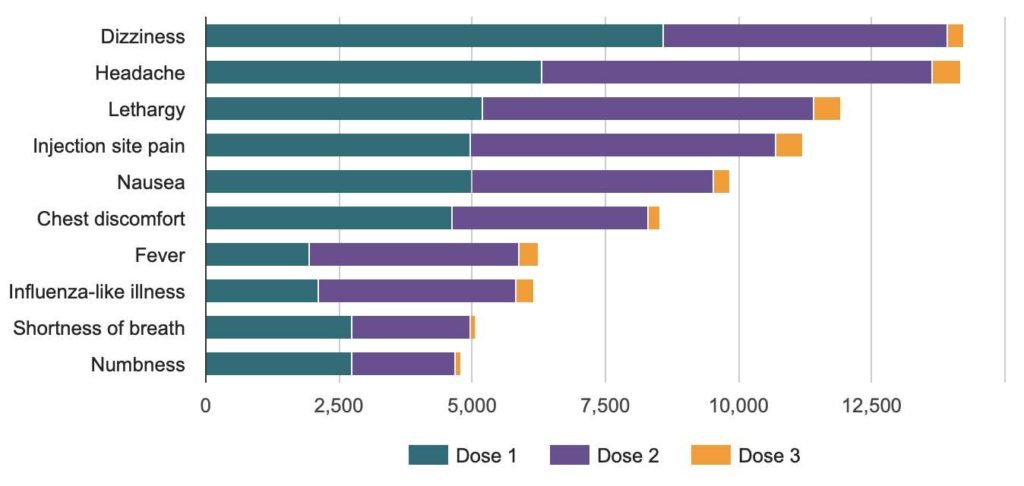
The ten most common adverse events
44,000 of the 46,000 adverse events are dismissed by Medsafe as ‘non-serious’—a number that has been echoed by politicians across the NZ political spectrum and by our Ministry of Health.
The prestigious Mayo Clinic in USA reported prior to the pandemic that the risk of developing myocarditis is rare and lists the following concerning symptoms of myocarditis:
https://www.mayoclinic.org/diseases-conditions/myocarditis/symptoms-causes/syc-20352539
Mayo Clinic—Myocarditis Symptoms
If you’re in the early stages of myocarditis, you might have mild symptoms such as chest pain, rapid or irregular heartbeats, or shortness of breath.
Some people with early-stage myocarditis don’t have any symptoms.
The signs and symptoms of myocarditis vary, depending on the cause of the disease. Common myocarditis signs and symptoms include:
- Chest pain
- Rapid or irregular heartbeat (arrhythmias)
- Shortness of breath, at rest or during activity
- Fluid buildup with swelling of the legs, ankles and feet
- Fatigue
- Other signs and symptoms of a viral infection such as a headache, body aches, joint pain, fever, child dizziness, a sore throat or diarrhea
Sometimes, myocarditis symptoms may be similar to a heart attack. If you are having unexplained chest pain and shortness of breath, seek emergency medical help.
Of the ten most common adverse effects of Covid-19 vaccination reported to CARM in NZ, you can see eight are listed as symptoms of myocarditis by the Mayo Clinic.
Given that myocarditis is the most common known severe outcome of Covid-19, why have the eight common vaccine adverse effects also known to be symptoms of myocarditis been characterised as ‘non-serious’?
Is this a glaring case of misdiagnosis? If so, why?
NZ GPs and Medical Personnel Had a Naive Expectation of Vaccine Safety
The first point to note is that most NZ doctors medical professionals had expectations of vaccine safety based on both years of experience with vaccination programmes and the extensive medical education they had received.
They had no prior experience with drugs or vaccines that had not already completed years of testing and safety evaluation.
It was for them therefore virtually unthinkable that the Pfizer vaccine was unsafe.
Moreover the Pfizer vaccine trial results had already characterised the common adverse effects as non-serious.
For this reason the very common reports of chest discomfort and shortness of breath following Covid-19 vaccination, which according to prior protocols should have led to intensive investigation and treatment, were dismissed as non-serious without investigation and in most cases without reporting to CARM.
Perhaps their very common occurrence fostered an attitude of indifference and dismissal which many victims suffered in NZ when they reported such symptoms to their GP or to hospital staff.
Rates of Myocarditis Symptoms are Higher Than Realised
The prevalence of a wide range of known myocarditis symptoms are probably indicative of a very high rate of subclinical and mild myocarditis following Pfizer vaccination.
The important point to note is that the recommended treatment for mild myocarditis is rest.
Most people recover if it is treated early with sufficient prolonged rest.
If left untreated, Myocarditis can restrict the capacity of the heart to pump blood which can lead to serious cardiac events such as heart attack, stroke, and arrhythmia.
It is contraindicated to undertake vigorous physical activity including sport while suffering from myocarditis.
It is clear from this that insufficient precautionary instructions were given to vaccine recipients about the risks they faced and the steps that they needed to take to avoid these risks.
This may have contributed to cardiac problems including among some recipients undertaking vigorous physical exercise.
The possible extent of these cardiac events is indicated by multiple reports to voluntary organisations such as NZDSOS and the Health Forum NZ.
An important point to note here is that reporting to CARM is not mandatory, a very unfortunate yet unforgivably deliberate omission.
Medsafe attempts in its Safety Report #39 (referenced above) to dismiss the significance of adverse events by comparing their rate to population norms.
In the absence of mandatory reporting, especially considering that Medsafe knows adverse events are grossly under-reported, all such comparisons are statistically meaningless.
A Public Information Campaign is Essential
Belatedly Dr Ashley Bloomfield, Director General of the Ministry of the Health, struck a note of alarm about myocarditis in his December 15 2021 letter to directors of DHBs, but this concern did not alter much the processes being applied.
Individuals experiencing myocarditis following their first vaccination are still being denied exemptions.
Those suffering strokes and heart attacks are in some if not most cases being denied Accident Compensation Commission (ACC) assistance.
There is also a virtual data black-out on rates of cardiac events and hospitalisations and on ACC claims.
Anecdotal and whistleblower reports here and overseas suggest these might be high but considering that data collection has been haphazard due to the non-serious label, these might be hard to quantify unless the government makes an honest attempt to inform the public of risks and ask people to come forward who are already affected.
This is particularly important as many stroke, cardiac and other serious adverse event sufferers have already been emphatically informed by their GP or other medical professionals that their symptoms must be unrelated to the Pfizer vaccination—an egregious form of victim blaming lacking any scientific basis.
Guy Hatchard PhD is formerly a senior manager at Genetic ID a food safety testing and certification company.
Media Representatives, this report is available as a PDF document, click here to view and or download A Report on the Interpretation of Covid-19 Pfizer Vaccine Safety











